
Comparison of Weight Loss Surgeries (Bariatric/Obesity Surgeries)
KR MANNUR, Consultant Bariatric Surgeon, London
This is only a rough guide. Discuss with your surgeon
|
Comparison of Weight Loss Surgeries (Bariatric/Obesity Surgeries) KR MANNUR, Consultant Bariatric Surgeon, London |
|---|
Type of Operation |
Restrictive and Malabsorptive |
Restrictive |
||||
|
Laparoscopic Roux-en-Y Gastric Bypass (RNYGB) or OAGB/MGB |
Laparoscopic Sleeve Gastrectomy (SG) with Duodenal Switch(DS) or SADI-S |
Sleeve/Tube/Vertical |
Laparoscopic adjustable gastric band (LAGB) |
||
What does the Operation entail? |
Thumb sized 12-15cm long stomach pouch connected to the small bowel. Food & digestive juices join about 1/3 the way down the small bowel i.e.1/3 small bowel and most of stomach is bypassed. |
Sleeve Gastrectomy performed first. The duodenum (first portion of the small bowel) is then connected to the last 300cm of small bowel. Food and digestive juices join in the last 75-100 cm of small bowel i.e. 3/4 of small bowel is bypassed. |
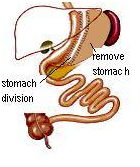
Stomach is divided vertically and 4/5 of the stomach (greater curve side) is removed leaving a long narrow tube with a capacity of about 75 cc (1/8 pint). Pylorus (the stomach outlet valve) is retained. No re-routing of bowel. |
An adjustable silicone ring (band) is placed around the top part of the stomach creating a small 15 cc pouch. |
||
Procedures |
One Anastamosis Gasric Bypass OAGB |
SADI-S |
Complete Uniform Sleeve – dividing stomach 1-3 cm from the pylorus to 1/2cm from the angle of His |
|
||
How does it works? |
· Significantly restricts the volume of food that can be taken. |
· Moderately Restricts the volume of food that can be taken. |
· Significantly restricts the volume of food that can be taken. |
· Moderately restricts the foods that can be taken. Doesn’t restrict sugary stuffs or liquids. |
||
How much Weight Loss is achieved? |
· 65% excess weight loss |
· 80-90% loss of excess weight |
· 65% excess weight loss at 2 years |
· 40-55% excess weight loss. |
||
Cured? When? |
Unrelated to wtloss1,4 |
Unrelated to wt loss 1,4 |
Totally weightloss-related |
Totally weightloss-related |
||
What Dietary Modifications should be made in the long term? |
· Patients must consume 3 small high protein (total 60gm/d) meals per day |
· Consumption of fatty foods causes diarrhea and malodorous gas/stool. |
· Must consume small amounts of food. Should stop eating once you feel full |
· Must consume less than fist size amount of food at any stage. Eat 3-4 times a day |
||
What Nutritional Supplements are required for life? |
· Multivitamins-B12,D |
· Multivitamins – B12,D |
· Multivitamins - B12, D |
· Multivitamins, D |
||
What are the Potential Problems in the long run and immediate peri-operative period? |
· Dumping syndrome |
· Nausea and vomiting |
· Nausea and vomiting |
· Slow weight loss/ very little weight loss (higher failure rate) |
||
Hospital Stay |
1-2 days |
1-2 days |
1-2 days |
1 day |
||
Time off Work |
1-3 weeks |
1-3 weeks |
1-3 weeks |
1-3 week |
||
Operating Time |
<1 hours |
1-1 ½ hours (2nd stage DS/SADI-S) |
½ - 1 hour |
½ hour |
||
What operation should you undergo to get the best result? |
· BMI 35 - 55 kg/m² *RGB Low maintenance, but has problems of dumping, ulcer, internal hernia requiring surgeries. Further surgeries for Weight gain difficult. |
· BMI >55 kg/m² *DS Low maintenance but require intense observation. May require surgeries for nutritional problems. SADI may have to be converted to DS for bile reflux |
· As ‘first stage’ in high risk or very heavy patients (BMI > 60 kg/m²) because of very low complication rate due to quicker operating time and recovery. *SG Very Very Low maintenance, but may require surgeries for acid reflux/ heartburn. DS/SADI can be added for weight gain |
· Best for patients who are well motivated and very disciplined in following dietary restrictions and exercise regime. * LAGB High maintenance. Problem with band fills. Complications high and require surgeries for complications and failure. 50% removed by 5 yrs, 65% by 7 yrs, & 100% by 10 years |
||
What makes the weightloss surgery safe? |
· Experience of the surgeon |
· Experience of the surgeon |
· Experience of the surgeon |
· Experience of the surgeon |
||




.png)