One Anastomosis Gastric Bypass OAGB / Mini Gastric Bypass MGB
What is One Anastomosis Gastric Bypass OAGB / Mini Gastric Bypass MGB
MGB or OAGB or Omega loop Gastric Bypass is good in patients where there is not much acid reflux. If the acid reflux is severe after the operation, then it has to be converted to RNY gastric bypass. It is more a malabsorptive operation than RNY gastric bypass. It is one anastomosis less and seems to give as much or even more weight loss than RNY Gastric Bypass; if nutritional problems become too severe, then the limbs have to be readjusted by surgery. It is said the internal hernias are much less (though can occur) and reversal to normal is easy.
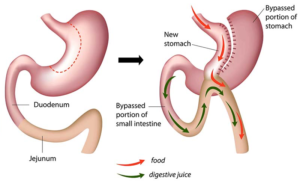
One Anastomosis Gastric Bypass OAGB/Mini-Gastric Bypass MGB or Omega Loop Gastric Bypass is basically bringing a loop of small bowel (Jejunum) and joining to Gastric pouch half the gastric bypass in that there is no Roux-en-Y formation of the gastric bypass. A loop of small bowel about 150-200cm (the length is increased in super obese patients) from the Duodeno-jejunal Flexure is joined to a long (20cm long) gastric pouch, without creating the RNY configuration, to create a 150-200cm afferent limb (Biliary Pancreatic limb). No further attempt is made to divert the bile and pancreatic juices away from the gastric pouch. The long length of the gastric pouch creates restriction almost like ‘gastric sleeve’. The long length of BP limb creates the malabsorptive component. So it is both restrictive and malabsorptive. It is better to do an endoscopy every 5 years to make sure that the bile reflux into stomach is not going into the oesophagus and causing any changes in the oesophagus; the bile amount will be much less because of the long length of the stomach pouch and the less amount of bile coming into the stomach itself because of the long Afferent limb (BP limb).
The rest of the metabolic effects are like the RNY Gastric bypass.